
“Content” has replaced “digital” as the biggest buzzword in marketing today—and is now at the core of all communications plans. According to a report by Accenture published late last year, 78% of pharmaceutical and biotech marketers now produce a “moderate to enormous” amount of digital content—from patient testimonials, social posts and news articles to shareable videos.
The truth is that content marketing can be one of the most effective ways to change audience behavior and move the needle on business objectives—but it can also easily fall flat. That’s why it’s more important than ever for marketers to develop clear objectives and strategies for their campaigns and avoid what I call the Seven Deadly Sins of Content Marketing.
SIN #1: You assume people care about your brand story
Let’s be honest; people don’t wake up saying “I’d like to sign a pledge today” or “I’d like to watch a patient video called Sam’s Story.” When developing content, you have to put yourself in the mindset of everyday people (yes: patients, caregivers, and healthcare professionals are people, too) and ask yourself a critical question: Why should they care? People are exposed to up to 10,000 brand messages a day, so for a brand to make an impact, its content has to be rooted in what people are already interested in, searching for and sharing.
Simply put, to work well, content must be as on trend as it is on message. Through social listening research, you can determine the conversations patients and healthcare professionals are already having about their condition and everything that surrounds it so you can enter those conversations authentically. For example, consider structuring your patient stories as listicles, hacks, and memes to build a library of valuable and snackable content that breaks through the clutter.
SIN #2: Your content is socially embarrassing
Every time we ask a person to engage on social platforms, we are asking them to do it publicly. While we work hard to remove the stigma from conditions like inflammatory bowel disease and vaginal atrophy, we have to recognize that there are just some aspects of people’s lives they don’t want to share in a public forum. Does that make social content off limits for conditions like these? No. But brands have to find ways to produce content that people would feel proud—or obligated—to share with other patients, caregivers and everyday friends.
For example, I helped develop a campaign for injectable dermal fillers. While millions of women use fillers, it remains a behind-closed-doors conversation because of the cultural bias associated with facial aging treatments, so we knew women would be hesitant to share social content. To overcome this, we tapped in to the pop-culture trend of mother-daughter “generation” photo shoots and asked daughters to re-create photographs of their mothers at the same age they are now to show how looks change as we age. The program sparked widespread engagement with consumers and media and authentically included discussion about treatment options to help women fight their genes and maintain natural-looking beauty as they age.
SIN #3: You are too focused on the subtleties of your execution
Pharma marketers already have enough hurdles to jump through to get their content out into the world. Obsessing about font type and rounded edges of photos that patients will never notice (or care about) just further delays getting content out while it’s still relevant.
Your attention is better spent on evaluating whether or not your content is relevant to information and conversations your target is interested in. Is it bringing real value to their life? Will they feel smarter, more hopeful and more connected after engaging with it? If the answer is “no,” then no amount of tweaking the color gradient is going make a difference.
SIN #4: Your content requires too much time and money
Authentic content that resonates isn’t always highly produced. In fact, very little sharable content is. Successful content strategies include a variety of production levels, so strike a balance between a well-produced “hero brand video” and a less expensive Instagram story. This will allow you to quickly enter conversations in real time and effectively use your budget to produce more content that keeps your brand top of mind (and top of feed).
I also believe it’s important to lean on agencies beyond your traditional ad agency for content. Your other partner agencies, including digital, social and PR, may have a stronger and more authentic way to understand what your patients are looking for and talking about and therefore can craft content that authentically engages, changes behaviors and moves your business.
SIN #5: You think that, if your content is good, it will get seen
Ensuring that your content is seen requires a mix of earned media attention and paid media boosting. For better earned media exposure, consider giving influencers and media a “first look” (before distributing it broadly to consumers), which can enhance its “hot off the press” appeal and incentivize them share it on their channels. Investigate partnerships with popular publishers to co-create content, which will give it even more credibility. Boost your content’s appeal through search optimization and simple but effective tactics like crafting a compelling title and robust description.
From the paid perspective, it’s important to remember that, for marketers, social media platforms are “pay to play.” There are very limited instances when your audience will see your content without paid support. My rule is to allocate at least 15% of the cost of the content for promotional dollars to ensure that even existing fans see it.
SIN #6: You are asking consumers to generate content for you
Let’s be real—how often do you “Share Your Story” on a social channel? Brands that set out to source real consumer stories as the cornerstone of their marketing campaign are destined to be disappointed in the results.
To make user-generated content (UGC) work for you, keep the following in mind:
- Tap in to moments when consumers are ALREADY sharing photos and videos, and ride that wave of existing conversations and content.
- Use an existing community of like-minded content creators to spread your story. You can access these through a myriad of vendors.
- Don’t underestimate the value of offering an incentive. Coupons, gift cards and surprise-and-delights don’t have to be expensive to be meaningful and compelling and can easily fall into pharma guidelines.
SIN #7: You give up on content because of regulatory hurdles
In a highly regulated environment, it’s understandable that pharma marketers throw up their hands in frustration when it comes to developing content and opt for an unbranded campaign that may not provide the same ROI. Good branded healthcare content requires incredible diligence. But it is possible.
Whether your content is branded or unbranded, you can help your program succeed by collaborating with your legal/regulatory team early in the process. To enhance compliance, consider using the latest platform tools like comment turnoff and static Important Safety Information on images and video, and keep up to date on the current cost-effective monitoring capabilities from your agencies and partners.
By keeping business objectives and consumer behavior top of mind, we can ensure that content does more than flood our feeds with more things to scroll past. There are many ways you can produce quality content that your target audience will want to see—and turn every post, every video, every story into an engine of conversation and engagement that drives your business forward.






 For the last two years, we have conducted a revealing survey among women making healthcare decisions asking how much they trust the pharmaceutical industry – the WEST Survey on Pharma: Women’s Engagement, Satisfaction & Trust. This year, we also conducted the same survey among 300 men, the MENT Survey on Pharma: Men’s Engagement, Needs & Trust, again through our subsidiary Health Stories Project, an online community of people inspired to tell their health stories to help others to connect and learn.
For the last two years, we have conducted a revealing survey among women making healthcare decisions asking how much they trust the pharmaceutical industry – the WEST Survey on Pharma: Women’s Engagement, Satisfaction & Trust. This year, we also conducted the same survey among 300 men, the MENT Survey on Pharma: Men’s Engagement, Needs & Trust, again through our subsidiary Health Stories Project, an online community of people inspired to tell their health stories to help others to connect and learn.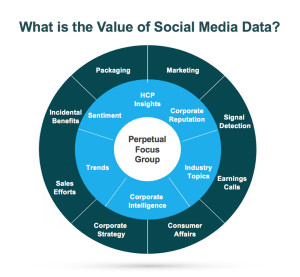 In the healthcare industry, patients and healthcare providers (HCPs) are looking to social media for information and support regarding their health and the health of their patients. They serve as a “perpetual focus group,” whose conversations taking place on social media provide brands with the opportunity to listen. Patients share their opinions, ask questions about diseases and treatment options, and directly or incidentally report adverse events. Meanwhile, HCPs voice opinions on the healthcare industry, provide thought leadership on a wide range of topics such as participatory medicine, reimbursement, and medical education. In a recent survey, more than 40 percent of respondents reported that information found via social media would affect the way they coped with a chronic condition or their approach to diet and exercise; 34 percent said it would affect taking certain medication.1 This demonstrates to companies that patients are directly impacted by what they view on social media and in order for brands to leverage that data radiating out of all the social conversations, several factors need to be in place.
In the healthcare industry, patients and healthcare providers (HCPs) are looking to social media for information and support regarding their health and the health of their patients. They serve as a “perpetual focus group,” whose conversations taking place on social media provide brands with the opportunity to listen. Patients share their opinions, ask questions about diseases and treatment options, and directly or incidentally report adverse events. Meanwhile, HCPs voice opinions on the healthcare industry, provide thought leadership on a wide range of topics such as participatory medicine, reimbursement, and medical education. In a recent survey, more than 40 percent of respondents reported that information found via social media would affect the way they coped with a chronic condition or their approach to diet and exercise; 34 percent said it would affect taking certain medication.1 This demonstrates to companies that patients are directly impacted by what they view on social media and in order for brands to leverage that data radiating out of all the social conversations, several factors need to be in place.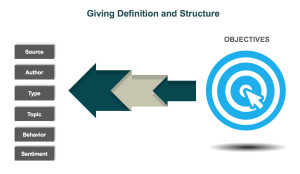 d is looking to identify who is talking about a product, the kinds of content they are posting, and the topics within their content, a structure that would classify posts into categories such as Consumer, Branded Product, and Medical Inquiry could be utilized. As more and more posts are tagged, patterns, trends, and themes can be identified.
d is looking to identify who is talking about a product, the kinds of content they are posting, and the topics within their content, a structure that would classify posts into categories such as Consumer, Branded Product, and Medical Inquiry could be utilized. As more and more posts are tagged, patterns, trends, and themes can be identified.